
Childhood hypertension serves as a critical predictor of hypertension in early adulthood, a condition that ranks as a leading risk factor for cardiovascular diseases and kidney disorders. Hypertension in children is defined as systolic or diastolic blood pressure reaching or exceeding the 90th percentile for their age, gender, and height based on normal-weight peers. The prevalence of this condition among adolescents is approximately 11%, with rates increasing alongside age and obesity levels. Key contributors to childhood hypertension include obesity, unhealthy diets, and physical inactivity, which are intricately linked to socioeconomic status and structural racism. This connection places a disproportionate burden on low-income and minority children, particularly non-Hispanic Black and Hispanic youth.Among non-pharmacological interventions, the “Dietary Approaches to Stop Hypertension” (DASH) diet is recommended. This approach emphasizes a high intake of fruits and vegetables, low-fat dairy products, and reduced sodium and saturated fat consumption. However, widespread adoption remains limited due to insufficient promotion. The 2010 Healthy, Hunger-Free Kids Act mandated improvements in the nutritional standards of the U.S. National School Lunch Program and Breakfast Program, aligning school meals more closely with the DASH diet and establishing them as a primary source of nutritious food for children. Despite over 28 million children participating in the National School Lunch Program, some families—whose incomes slightly exceed free or reduced-price eligibility thresholds or who fear stigmatization—fail to fully utilize this resource.The Community Eligibility Provision (CEP) addresses this gap by allowing schools with a high proportion of low-income students to offer free breakfast and lunch to all students, significantly boosting participation rates and dietary quality. Since its nationwide expansion in 2014, over 47,000 schools have adopted CEP by 2024, benefiting more than 23 million children. Beyond federal initiatives, several states have independently promoted universal free meals during and after the pandemic. Given the increasing adoption of these policies, evaluating their health impacts is crucial. CEP holds the potential to lower childhood hypertension risk by improving nutrition, reducing obesity, and alleviating financial strain and food insecurity for families.

This study employed a difference-in-differences design, utilizing electronic health record (EHR) data from the Community Health Organizations (OCHIN) Network in 12 US states between 2013 and 2019. The study matched patients’ home addresses to schools and examined the association between school participation in the Community Health Program (CEP) and student blood pressure outcomes. The study included children aged 4 to 18 years, taking into account patient demographics (age, sex, race/ethnicity, health insurance status) and state Medicaid expansion policies. Statistical models controlled for time-invariant school characteristics and potential confounders to assess the causal impact of the CEP policy. The primary outcome measure was the proportion of patients with blood pressure exceeding the 90th percentile per school per school year. Secondary outcomes included blood pressure reaching the hypertension threshold (95th percentile) and mean systolic and diastolic blood pressure percentiles.
Results: 1,052 schools and 155,778 patients were included. The majority of students in these schools were from low-income families, and the racial composition was primarily Hispanic (46%), non-Hispanic Black (13%), and non-Hispanic White (25%). Among students in schools participating in the CEP, the proportion of students with blood pressure above the 90th percentile decreased significantly compared with students in non-participating schools, with an average reduction of 2.71 percentage points (95% confidence interval, −5.10 to −0.31), corresponding to a total net reduction of 11% over five years.
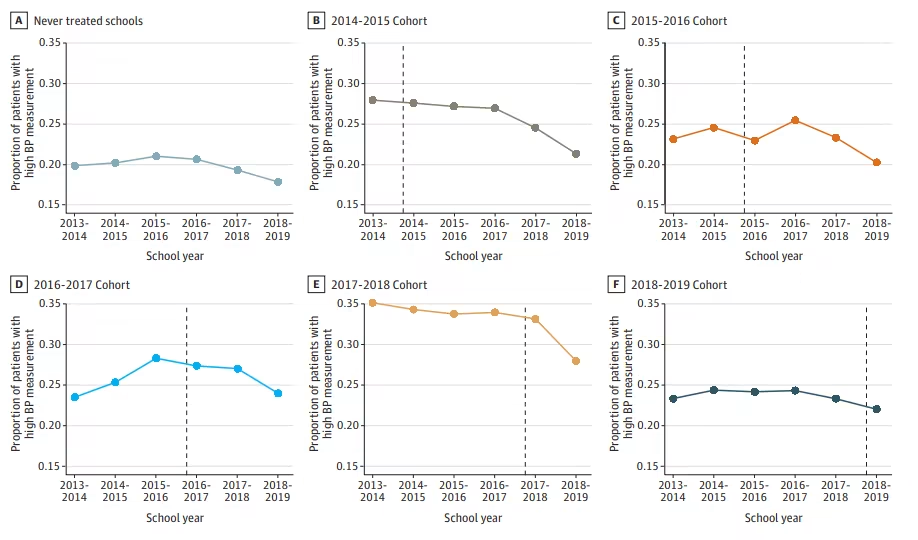
Unadjusted trends in the proportion of patients with elevated blood pressure measurements, by year the school adopted the community eligibility provision
In summary, this study’s evidence supports the positive effects of universal free school meal policies on improving children’s blood pressure. CEP may effectively reduce the risk of hypertension by increasing school meal attendance, improving diet quality, reducing obesity rates, and alleviating household food insecurity. Such policies may help mitigate health inequalities, particularly among low-income and minority children. Schools that adopt CEP early experience greater blood pressure improvements due to the longer-term benefits. Although the prevalence of hypertension in US children has increased, the recent trend may be declining. Future research should examine the impact of improved school meal nutrition standards and the expansion of CEP on long-term trends in children’s blood pressure.
Original Source
Localio AM, Hebert PL, Knox MA, et al. School Provision of Universal Free Meals and Blood Pressure Outcomes Among Youths. JAMA Network Open. 2025;8(9):e2533186. doi:10.1001/jamanetworkopen.2025.33186
The academic information for this article was provided by Mays Medical. This article was translated using an independently developed AI academic robot and then proofread by a clinician. If any content is inaccurate, please leave a message.
Leave a Reply